Home
Home Health
Health Diet & Nutrition
Diet & Nutrition Living Well
Living Well More
MoreMalignant hyperthermia or MH is a rare inherited disorder. MH causes a hypermetabolic, life-threatening reaction in the skeletal muscles called a fulminant MH event. Doctors classify malignant hyperthermia as a pharmacogenetic disorder because volatile anesthetics or polarizing skeletal muscle relaxants almost always trigger the events. A fulminant MH event may be triggered by stress, exercise, or high environmental temperatures, although this is very rare. If medical practitioners cannot take immediate action to halt and treat fulminant MH episodes, the fatality rate can be as high as 70%. The risk of fatality is higher for children.
Signs and Symptoms of Malignant Hyperthermia
Signs of malignant hyperthermia include muscle rigidity, an excessively high body temperature, and rapid heart rate. Other indicators of a fulminant MH event are increased acid content in muscles and carbon dioxide build-up in the blood. The onset of a fulminant MH event can occur within minutes or hours of a patient receiving anesthesia.

Fulminant Malignant Hyperthermia
Each episode of fulminant malignant hyperthermia is different. A person can have a fulminant MH event even after successfully tolerating anesthesia in previous procedures. Medical professionals must always be alert for MH. People may show different symptoms, and it is the responsibility of anesthesiologists and care providers assisting the surgeon to watch for signs of MH and notify the specialist immediately. After a person who experienced an MH event stabilizes, the doctor will take a muscle biopsy for testing.

Genetics and Inheritance of Malignant Hyperthermia
The genetic mutation responsible for malignant hyperthermia is an autosomal-dominant trait. This means that a person has the disorder when they inherit just one copy of the mutated gene from either parent. MH affects men and women equally, and the risk of passing the mutated gene to offspring is 50% for each pregnancy. Mutations in the CACNA1S gene can also result in malignant hyperthermia, but CACNA1S accounts for less than 1% of all cases.
Mechanism of Action
Malignant hyperthermia is the result of an abnormal type 1 ryanodine receptor calcium release channel gene on chromosome 19 called RYR1. The receptor controls calcium regulation within muscle cells. An abnormal receptor causes a build-up of calcium ions within cells. The triggering substance initiates an uncontrolled release of calcium ions, which triggers pumps within the cells to transport the excess to extracellular spaces. The skeletal muscle cells use a huge amount of cellular energy or ATP to regain equilibrium and control of the calcium ions. The heat produced from excessive energy use within cells damages muscle cell membranes and results in hyperkalemia and rhabdomyolysis. Hyperkalemia is excessive potassium in the bloodstream and causes rapid, irregular heart rate.
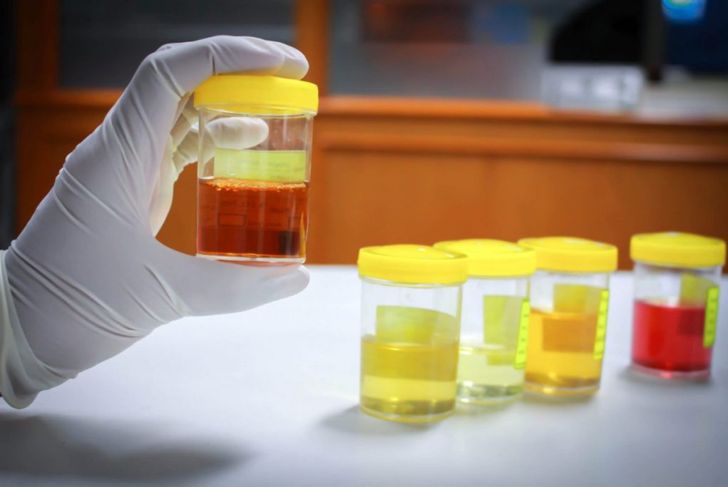
Rhabdomyolysis
Rhabdomyolysis is the medical term for rapid breakdown of skeletal muscle. Symptoms include muscle pain, weakness, vomiting, irregular heartbeat, and confusion. Dark brown tea-colored urine is a characteristic sign of rhabdomyolysis. The urine color comes from the presence of the protein myoglobin and other products of muscle breakdown. Kidney failure is possible from the influx of large proteins.
Hyperthermia
Muscles contract continuously during fulminant MH events. Contractions and energy use produce hyperthermia, which may occur later in the fulminant MH event or immediately. Severe hyperthermia at or above 113°F results in increased oxygen use and carbon dioxide production. Unchecked hyperthermia leads to widespread organ failure and coagulation within blood vessels.
Pediatric Malignant Hyperthermia
Children experiencing fulminant MH events have slightly different symptoms than adults do. The most common sign is a rapid and irregular heart rate. Hyperthermia and hyperkalemia occur faster, and potassium levels in the blood reach higher levels, in children than adults. Muscle rigidity occurs during approximately half of fulminant MH events in children under the age of 12. Younger children are more likely to have skin mottling with dark red and purple coloration. Children between the ages of 12 and 18 are three times more likely to have masseter muscle rigidity, which prevents the mouth from opening.

Incidence
Surgeons report a suspicion of malignant hyperthermia in 1/4 of procedures using general anesthesia. Suspicion means there were symptoms observed that may have signified malignant hyperthermia but did not progress to a fulminant MH event. A fulminant MH event is reported in approximately 200 out of 250,000 procedures under general anesthesia. These numbers are estimated loosely because doctors may report mild fulminant MH events as suspicions instead of confirmed occurrences. Variants of the RYR1 gene are present in approximately one out of every 2,000 people, although ongoing research suggests that the number of people with mutations of the RYR1 gene may be higher than previously thought.
Diagnosis
Many people with MH are not aware of it and have no symptoms. It is difficult to identify people at risk of a fulminant MH event before a procedure under general anesthesia. Family history is important because MH is an autosomal-dominant inherited disorder. A CHCT test in North America or an IVCT test in Europe will confirm the diagnosis. Both tests are done with biopsied leg muscle in MH diagnostic centers. Genetic testing is available as well.
Treatment
Recovery from a fulminant MH event depends on how medical professionals identify and treat the event. The medical team will immediately cease anesthesia administration and replace the substance with intravenous opiates and sedatives. Nondepolarizing muscle relaxants can enable the team to continue anesthesia if necessary. Researchers have identified one specific drug as an antidote for anesthesia-induced fulminant MH. Doctors give the person experiencing the MH event 100% oxygen, and administer the antidote intravenously every five minutes until the person stabilizes. Side effects after rapid treatment include difficulty breathing, nausea, vomiting, headache, dizziness, and tissue death at injection sites due to incorrect administration of the injections. Side effects rarely occur after intervention.